Connectomics in Stroke

In order to understand what influences long-term outcome and can potentially improve it, a baseline of what to expect after stroke is essential. This baseline is, in principle, what one would expect even without intervention. A lot of work has already gone into understanding how brain structures influence outcome, which we have also looked into.
Brain connectivity is a novel analyses technique, which aims to describe how separate regions in the brain communicate with one another. It allows us to assess the efficacy of information transport in the brain, which is a key building block of how perform any kind of action in our daily lives. The combination of stroke outcome research and brain connectivity is therefore very intuitive.
Rich-club importance for stroke outcome
One key finding in brain connectivity is the so-called rich-club, a set of regions that is key for efficient functioning and infromation processing in the brain, acting as a high capacity backbone system. Van den Heuvel and Sporns identified 12 regions within the brain belonging to the rich-club (six per hemisphere). Additional studies have further investigated and demonstrated the importance of the rich-club in development, the healthy population, as well as during disease.
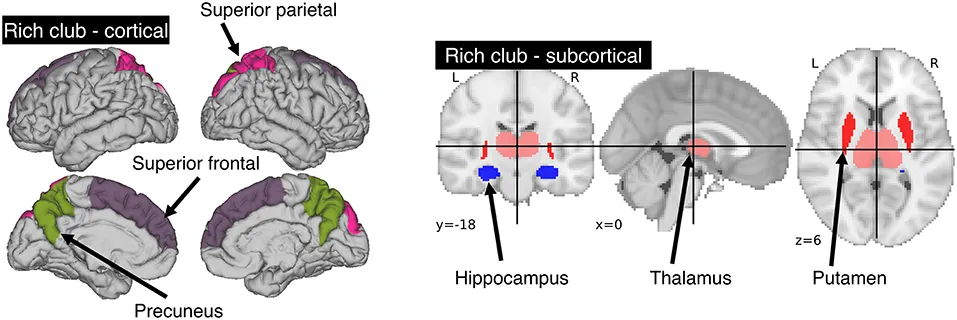
By incorporating structural connectivity information from healthy participants, specifically the location of the rich-club, we demonstrated that specific areas in the brain that are important for efficient information transport, have a much higher contribution to the patients outcome. Utilizing the GASROS study, we automatically determined how many of the rich-club regions were affected by the stroke (NRC) in clinical data.
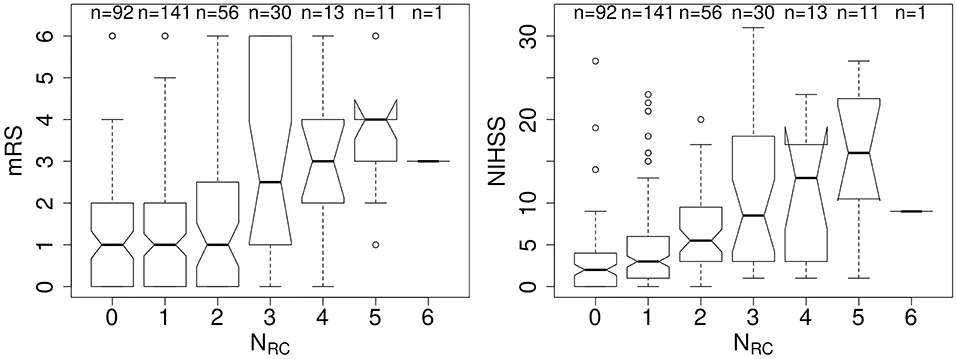
This allowed us to show the connection between this number, stroke severity (National Institute of Health Stroke Scale; NIHSS), and long-term outcome (modified Rankin Scale; mRS), as illustrated in the figure above. In our analysis, we showed that this simple assessment as a biomarker exceeds traditional markers such as lesion volume or age. Moreover, this solidifies the claim that the rich-club is crutial for effective and healthy functioning of the human brain. A full description of this work is openly available in the corresponding publication Rich-Club Organization: An Important Determinant of Functional Outcome After Acute Ischemic Stroke.
Rich-club and the added benefit of functional connectivity
Using an independet cohort, the SALVO study, we were able to reproduce our findings from the rich-club, while further expanding this concept. The SALVO study is quite unique, as the stroke patients underwent functional MRI in the early stages of the stroke, with detailed outcome measures. This allowed us to significantly improving our understanding of how structural and functional connectivity in the brain play a key role for stroke patients.
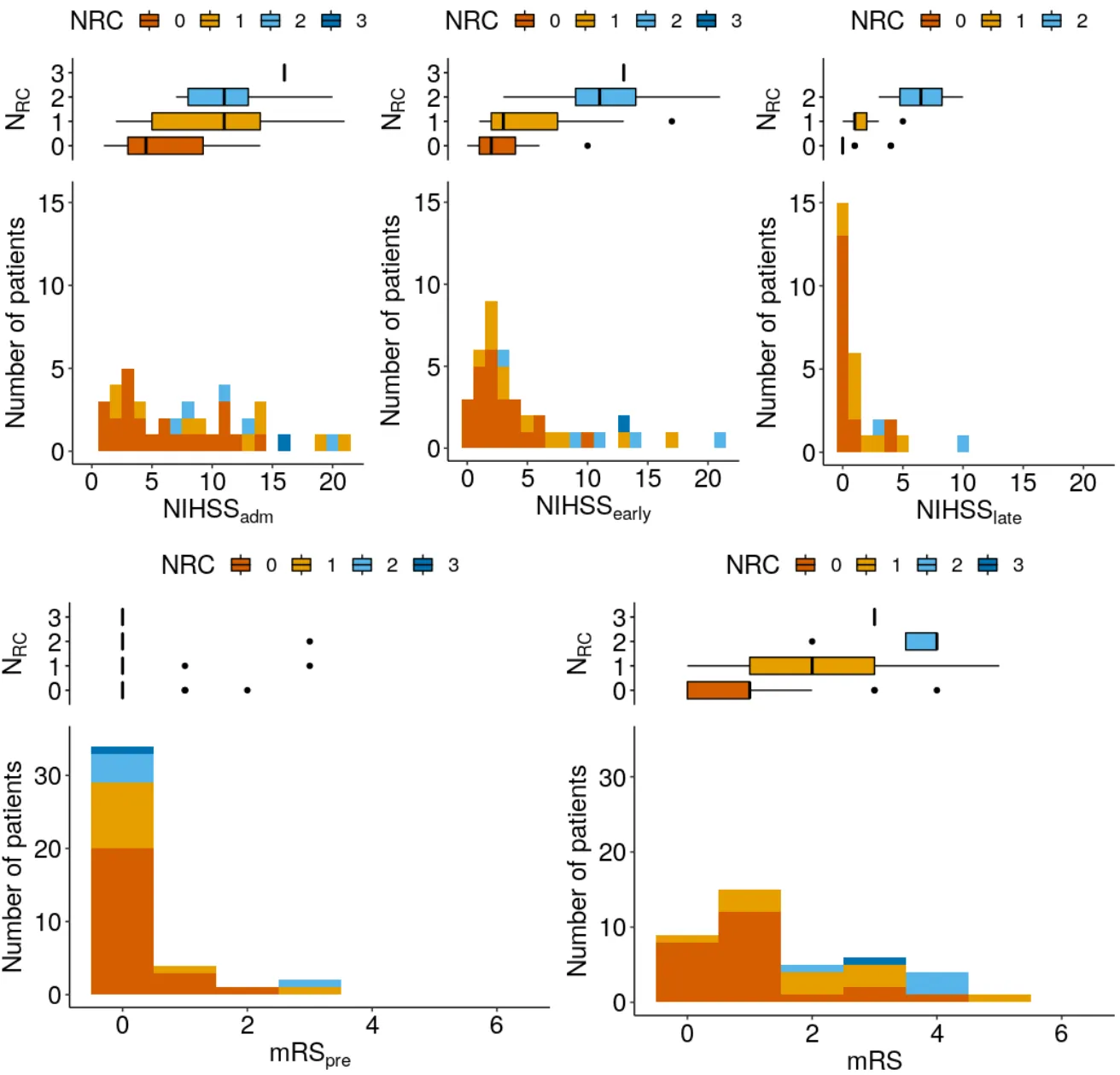
The figure above demonstrates the distribution of the patients in the SALVO study and their outcome pre-stroke (modified Rankin Scale; mRSpre), stroke severity at time of admission (National Institute of Health Stroke Scale; NIHSSadm), stroke severity in the early stages (NIHSSearly), as well as stroke severity (NIHSSlate) and mRS at approximately 3 months. We see similar tendencies as in the rich-club investigation above, where the more rich-club regions are affected by the stroke, the worse the patients outcome will be.
Utilizing the functional connectome infromation, we were able to show that incorporating modern analyses techniques from brain connectivity analyses, further improved our understanding and the ability to model of stroke outcome. Including the number of rich-club regions affected, we calculated a measure of efficiency within the function connectome, specifically the characteristic path-length (see background section for more information). As a quick summary, our outcome model including both the rich-club and the functional connectome infromation, we showed an 1.3 - 2.6-fold increase in our ability to explain the observed outcomes, beyond traditional markers such as age and the size of the stroke. More details can be found in our publication "Brain connectivity measures improvemodeling of functional outcome after acuteischemic stroke".